Benign Tumors
Jaw tumors are often benign and grow slowly, but can disrupt surrounding tissue and are often detected via X-ray. Diagnosis is made with a biopsy, and treatment can range from observation to surgery. Innovative methods like stem cell-generated bone and titanium implants improve outcomes.
Table of contents
This article is based on an original article in Swedish which can be found here
BACKGROUND
The term tumor refers to a tissue neoplasm (swelling or lump) and has its linguistic origin in the Latin word tumor. This tissue neoplasm, which is sometimes also referred to as a neoplasm, rarely or never has any physiological function but can increase in size more or less continuously over time, independent of the growth of other adjacent tissues.
When a tumor is benign, it means that it does not produce daughter tumors (metastases) and generally, with certain exceptions, respects anatomical boundaries, unlike malignant tumors that invade surrounding tissues and also have the capacity to metastasize to other locations in the body. However, benign tumors can cause damage by affecting other structures through pressure, or the tissue around the tumor may be resorbed to make room for the process. Benign tumors can also, through their growth pattern, give rise to progressively increasing asymmetries (differences in appearance between the affected and healthy side).
A characteristic of a benign tumor is that they are always composed of "normal" cells, that is, cells that are more or less fully differentiated or mature. Furthermore, benign tumors are often named based on the tissue from which they originate, for example, ameloblastoma, which originates from the enamel-forming ameloblasts, or osteoma, which originates from bone tissue.
The benign tumors found within the confines of the jaws are a heterogeneous group and are relatively rare. Figures of up to 3% of all oral pathological tissue samples and up to 0.003% of all tumors in the body have been described in the literature.
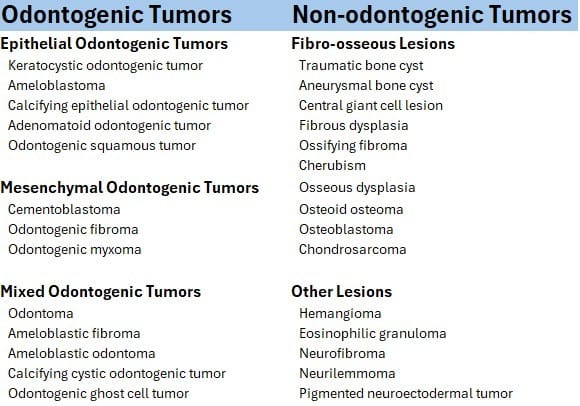
Classically, jaw tumors are divided into odontogenic and non-odontogenic tumors (Table 1), meaning whether they originate from the tissues that give rise to teeth or not. Purely odontogenic tumors are seen only in or in direct connection with the jaws, while non-odontogenic tumors are more often found in other parts of the skeleton. A revision of the WHO's previous classification of tumors found in the jaws was made in 2005 and is now based not only on histological characteristics but also on epidemiology, etiology, localization, genetics, and prognosis. This classification is updated regularly and has included that the keratocystic odontogenic tumor is now once again regarded as a cyst and has been excluded from jaw tumors.
The genetic origin of jaw tumors is complex and largely unexplored, but several molecules that can influence tumor development and progression have been identified, such as the oncogenes Ras, Myc, and Fos, the oncoviruses HPV and EBV, as well as interleukins 1 and 6. Mutations in the BRAF protein have also been identified in ameloblastoma and may be significant for prognosis assessment and treatment of potential recurrences. As advances are made in the genetic field, further revisions of the classification are likely to occur, and causes of tumor formations will be identified.